Squamous cell carcinoma of the EyelidDefinition: malignant neoplasm arising in and with differentiation toward stratified squamous epithelium
Incidence/Prevalence: Squamous cell carcinoma is at least 10 to 40 fold less common than
basal cell carcinoma in the eyelids, which accounts for about 90% of eyelid primary maligancies. Squamous carcinoma is the third most common eyelid malignancy accounting for about 4% of all primary eyelid malignant neoplasms.
Sebaceous carcinoma accounts for slightly more (5%).
Etiology: UV radiation is a clear factor in the cause of squamous cell carcinoma of the eyelid. The majority of squamous cell carcinomas arise in solar-damaged skin and premalignant lesions (actinic keratoses). Mutations of p53 are high in patients with actinic keratosis. One theory is that the formation of pyrimidine dimers from UV radiation in the p53 gene results in the inability to produce cell-cycle arrest in G1. The absence of cell cycle arrest impairs repair and/or elimination of damaged DNA and division continues of the mutant cells.
Clinical Findings: The clinical appearance is diverse, ranging from ulcers to plaques to fungating or nodular growths. The lower eyelid is more frequently involved than the upper.
Histopathology: The criteria for the diagnosis include atypical squamous cells forming nests and strands and infiltrating the dermis with squamous differentiation.
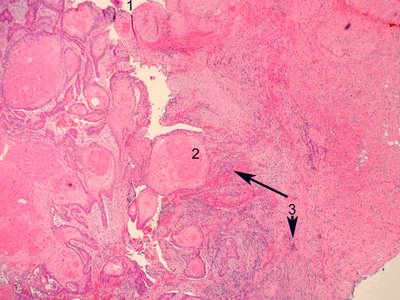
In the accompanying image, surface ulceration is evident (number 1). Large nests of well differentiated squamous epithelium with central keratin (keratin pearls)are present (number 2). Strands and isolated nests of malignant cells infiltrate the dermis (arrows 3).
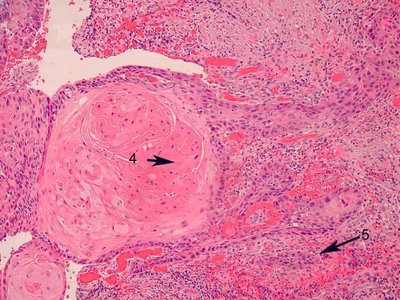
At higher magnification (middle image) the central keratin in the pearl is more visible (arrow 4) and strands of infiltrating atypical squamous epithelium (arrow 5) extend into the dermis.

At high magnification, (lower image) the central keratin in the dyskeratotic whorl of cells is obvious (arrow 6) and intercellular bridges (desmosomes or epithelial attachments) can be best visualized in edematous areas between cells as very thin lines attaching adjacent cells (arrow 7). Occasional mitotic figures are evident (arrow 8). In this series the extensive squamous differentiation in the form of keratin formation, pearls, and intercellular bridges indicate a well differentiated squamous carcinoma.
Treatment: Complete excision of the tumor is considered the best treatment and in small lesions may be curative.
Prognosis: Squamous carcinoma may invade perineurally and through lymphatics. Regional lymph node metastasis is reported to occur in 1%-21% of patients with squamous cell carcinoma of the eyelid.
